Kawasaki Disease: A Comprehensive Overview. Dr. Narmin Azizova

Dr. Narmin Azizova
Neonatologist, Department of Neonatal Resuscitation and Intensive Therapy, Scientific Research Institute of Pediatrics named after K.Y. Farajova; Department I, Azerbaijan Medical University; Founder, Pediatriya.az
General Information
Kawasaki disease is a systemic vasculitis affecting medium-sized arteries, primarily targeting the coronary arteries that supply blood to the heart. It predominantly affects children between 6 months and 5 years of age.
The exact cause of Kawasaki disease remains unknown, but it is believed to have a genetic predisposition. In addition, viral infections and environmental factors may contribute to its onset. Epidemiological data indicate a higher prevalence in males than females, with seasonal peaks observed in winter and spring [1,2].
Clinical Manifestations
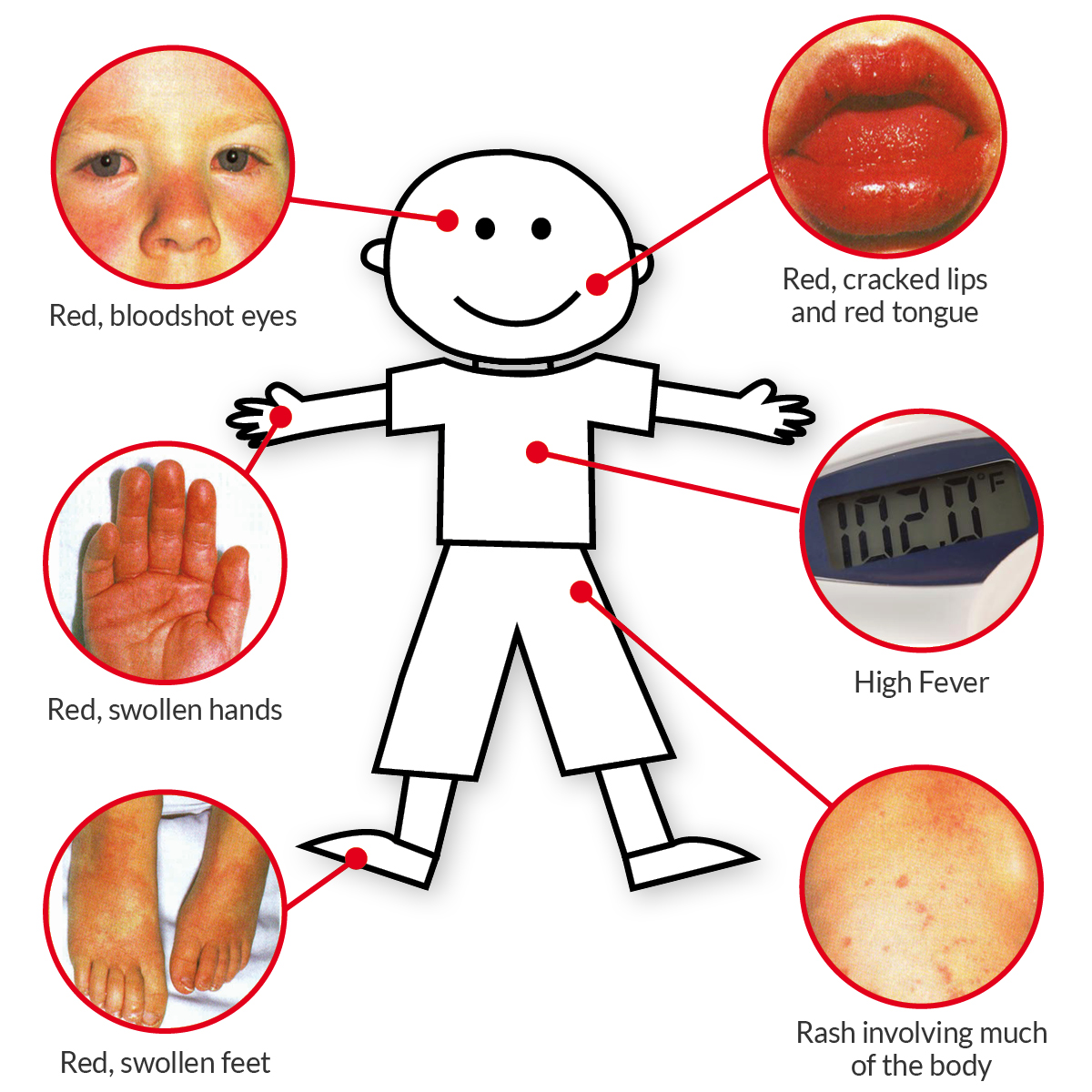
A persistent fever lasting more than five days that does not respond to antipyretic medications is a hallmark of Kawasaki disease. Additional key symptoms include:
- Bilateral non-exudative conjunctival injection (redness in both eyes without discharge)
- Cervical lymphadenopathy (typically unilateral and >1.5 cm in size)
- Oropharyngeal changes such as cracked, bright red lips and a swollen, “strawberry” tongue
- Polymorphous rash that often spreads from the torso to the extremities, sometimes involving the genital area
- Extremity changes, including palm and sole edema in the acute phase, followed by periungual peeling of the fingers and toes in the subacute phase
The diagnosis is confirmed when a child presents with at least four of the five major criteria along with prolonged fever [3].
One characteristic sign not included in diagnostic criteria but often observed is erythema and induration at the Bacillus Calmette-Guerin (BCG) vaccination site.
Additional symptoms may include arthritis, diarrhea, vomiting, and abdominal pain. If no complications arise, symptoms gradually subside.

Variability of the Disease
The severity of Kawasaki disease varies among individuals. Coronary artery aneurysms (CAAs) develop in approximately 2–6% of treated cases and up to 25% of untreated cases [4]. Infants under 12 months of age may present with incomplete Kawasaki disease, where not all typical signs are evident.
Kawasaki Disease and COVID-19
While most children experience mild symptoms of COVID-19, a small proportion develop severe complications such as Multisystem Inflammatory Syndrome in Children (MIS-C), which shares clinical features with Kawasaki disease. Some cases of MIS-C present with severe cardiac involvement, resembling Kawasaki disease, including coronary artery dilation or aneurysms [5].
Diagnosis
There is no specific laboratory test for Kawasaki disease; diagnosis is clinical. However, supporting tests include:
- Complete blood count (CBC): Leukocytosis, thrombocytosis, anemia
- C-reactive protein (CRP) & Erythrocyte sedimentation rate (ESR): Elevated inflammatory markers
- Urinalysis: Sterile pyuria
- Electrocardiogram (ECG): May show arrhythmias
- Echocardiography: Assesses coronary artery involvement
- B-type natriuretic peptide (BNP): Increased levels indicate cardiac stress
Complications
Kawasaki disease is the leading cause of acquired heart disease in children. Potential cardiac complications include:
- Coronary arteritis
- Myocarditis
- Valvular heart disease
- Coronary artery aneurysms, which may lead to myocardial infarction or life-threatening hemorrhage
Mortality is rare but can occur due to coronary complications if untreated.

Treatment Guidelines
Early treatment is crucial to prevent cardiovascular complications. Current American Heart Association (AHA) and European Society of Cardiology (ESC) guidelines recommend:
- Intravenous immunoglobulin (IVIG): Administered at a dose of 2 g/kg within the first 10 days of illness to reduce coronary artery complications.
- Aspirin therapy: High-dose aspirin (80-100 mg/kg/day) during the acute phase, followed by a lower dose for anti-inflammatory and antiplatelet effects.
- Corticosteroids or additional immunomodulatory therapy in IVIG-resistant cases.
- Long-term cardiac monitoring: Follow-up echocardiography at 6–8 weeks and 6 months post-diagnosis [6,7].
Post-Treatment Considerations
Children treated with IVIG should delay live vaccinations (e.g., varicella, measles) for at least 11 months, as IVIG can interfere with vaccine-induced immunity.
Sports and Physical Activity
Most children recover completely and can engage in normal physical activities. However, those with cardiac involvement should be evaluated by a pediatric cardiologist before resuming intense physical activity.
References:
- McCrindle BW, Rowley AH, Newburger JW, et al. Diagnosis, Treatment, and Long-Term Management of Kawasaki Disease: A Scientific Statement for Health Professionals from the American Heart Association. Circulation. 2017;135(17):e927-e999.
- Burns JC, Glodé MP. Kawasaki syndrome. Lancet. 2004;364(9433):533-544.
- Sundel RP. Kawasaki Disease. Rheum Dis Clin North Am. 2015;41(1):63-73.
- Newburger JW, Takahashi M, Gerber MA, et al. Diagnosis, Treatment, and Long-Term Management of Kawasaki Disease. Pediatrics. 2004;114(6):1708-1733.
- Feldstein LR, Rose EB, Horwitz SM, et al. Multisystem Inflammatory Syndrome in U.S. Children and Adolescents. N Engl J Med. 2020;383(4):334-346.
- AHA Scientific Statement: Diagnosis, Treatment, and Long-Term Management of Kawasaki Disease. Circulation. 2017.
- European Society of Cardiology (ESC) Guidelines on Pediatric Cardiac Conditions. Eur Heart J. 2022.